careoxyhealthservice's blog
Nasogastric (NG) and Ryles tubes are vital in the administration of appropriate, safe and comfortable care to patients with compromised eating or swallowing ability due to illness, surgical post-care or other causes. Nasogastric tubes inserted through the nose to the stomach, for feeding and also available for medications administration or even gastric decompression. In this detailed blog, we will go through the applications, dogma, and practices of NG tubes and Ryles tubes, especially their use in home feeding & medical care.
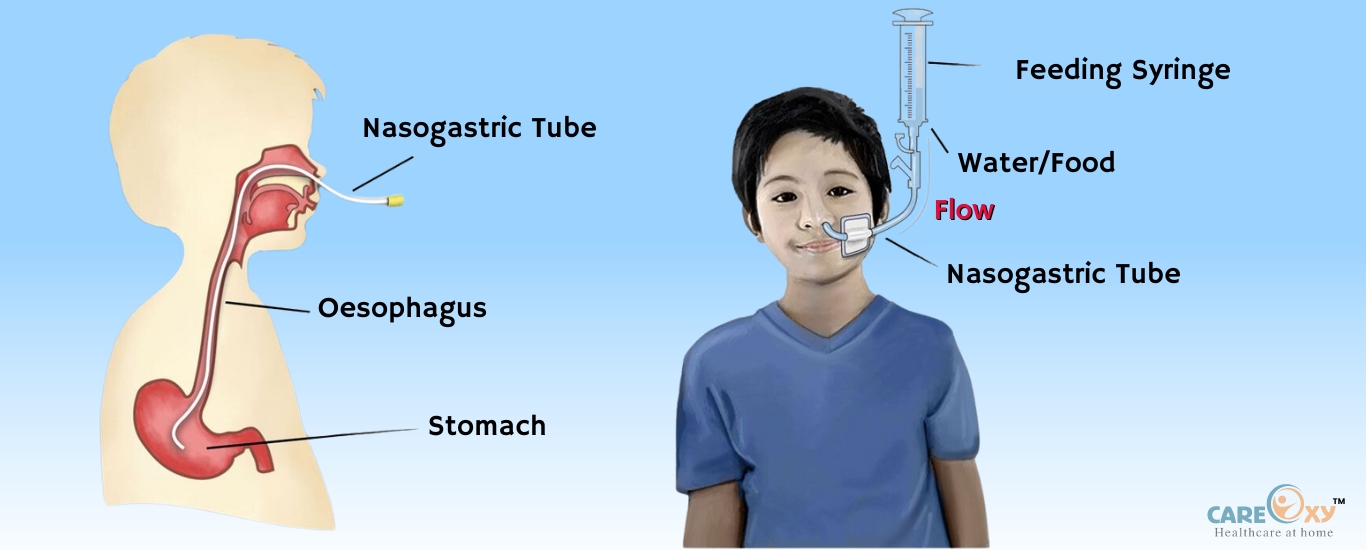
A nasogastric tube (NG tube) is a small, soft tube inserted through the nostril and cane or down into the oesophagus to the stomach. A tube through which the healthcare provider can put food, water, and medication into the stomach by going around your mouth and throat. It also gives you a conduit for aspirating stomach content such as in cases of bloating, nausea or other bowel-related complications where gastric decompression is needed.
Various sizes and types of NG tubes are available according to the patient's needs. These serve as short-term or long-term care based on the patient's condition.
What Is a Ryles Tube?Ryles tube is a type of nasogastric tube named after the English surgeon Sir Harford Ryles, who described it. This tube is more commonly used for decompression and its name might come up when doing clinical postgraduate studies this is also called as Ryles. although it serves similar purposes to the NG tube. feeding, decompressing. The difference between an NG tube and a ryles tube is pronounced so that sometimes the terms are wanted to be synonymous, though the Ryle's tube is characteristically stiffer.
Since, they were called NG and Ryles tubes… Main Uses of Nasogastric (NG) and Ryles TubesNG and Ryles tubes are the backbone of hospital as well as home-care scenarios. Something that I found to be interesting was the use of these tubes.
1. NUTRITIONAL SUPPORT AND FEEDING
NG tube feeding is necessary for patients who are unable to swallow due to conditions such as stroke, neurological impairment or esophageal injury. Liquid nutrition is delivered straight to the stomach, providing calories and nutrients needed for health.
Enteral feedings are this type of feeding, and NG tubes are one of the most commonly used devices for short term enteral nutrition. The tube feeding formula can be tailor-made depending on the patient's nutritional requirements and usually is prescribed.
2. Administration of Medications
Medication NG and Ryles tubes (tube through which medication is given directly to the stomach). This technique can be especially useful when a patient cannot swallow pills or liquid meds. Most oral medications can be crushed or dissolved and delivered through the NG tube, but this should be done with care to prevent tube blockage. Whenever Possible use liquid medication
3. Gastric Decompression
Decompression (NG / Ryles): Patients with a history of Bowel obstruction, Gastric bloating, and retained stomach contents can be decompressed using nasogastric tube/ryles tube. The goal is to remove surplus stomach gas and liquids so you will likely feel better due to nausea, retching, bloating etc., with the tube being attached to suction.
This usage is most common in instances of intestinal obstruction, postoperative ileus or for patients who are unable to tolerate nutrition orally. The tube keeps patients from being able to vomit, which stops aspirations that can worsen the lungs and can cause a very nasty pneumonia.
4. Gastric Lavage
Gastric lavage:It is also known as the stomach pump and it can be done by an NG tube. This is usually done as an emergency measure(in case of poisoning or drug overdose) to remove toxic substances from the stomach as soon as possible.
Procedure & Techniques in NG Tube InsertionThe insertion of an ng tube insertion is a medical procedure and should be done with skill and precision. Trained healthcare professionals can provide it at the hospital or in a home setting.
1: Preparation: The medical professional will collect the supplies and approach materials required to perform the procedure and they are NG tube, lubricating gel, syringe, gloves and tape for putting the tube into place. A. Medical HX: Review the pts medical record to make sure that there are no contraindications for NG tube placement (nasal obstruction, recent esophagectomy etc.).
The patient is placed in a high-Fowler's position (sitting upright at 45- to 90-degree angle) to help with insertion and lower the risk of aspiration. A large towel is wrapped around the patient's neck to avoid vomiting or choking.
Measuring the Tube: The healthcare provider will check the length of the tube by placing the tip over out of the nostril, over ear, and then down to the xiphoid process (the lower end of the sternum) to ensure that it goes into the stomach. This measures that the tube is long enough to reach the stomach but not too short to hang up in the oesophagus.
Lubricating the Tube:Ensuring the insertion is as smooth and comfortable for the patient as possible, lubrication is key. Water-soluble lubricant is placed onto the tip of the tube to enable it to glide down through the nasal passage and into the oesophagus.
Insertion: The NG caregiver then inserts the lubricated tube, which has been desired by the patient, into one of the patient nostrils. When this happens, the patient has to swallow or sip a little water to allow the tube to pass through the oesophagus. This step reduces as much as possible any associated discomfort and ensures that the tube is positioned correctly.
Verification of Tube Placement:This means that once the tube is in, it is necessary to ascertain that it is in the stomach and not in the lungs where it would pose a danger of aspirating, which is very dangerous. There are several techniques employ to check placement as follow:
Securing the Tube: Once confirmation of the proper placement has been made, the tube is retained onto the patient’s face by the use of adhesive tape. Depending on the reason for which the NG tube was placed, the outer end of the tube is fixed into a feeding pump, a syringe or even a suction machine.
Ryles Tube InsertionThe technique of inserting a Ryles tube is comparable to that of an ordinary nasogastric tube insertion
although the Ryles tube is, however, former thus causing some discomfort during introduction. Feeding and decompression are also indicated with the ryles tube insertion as with the NG tubes, although it is more often used when the purpose of these tubes is decompression or fostering gastric drainage.
Nasogastric Tube Feeding: Procedure and Best PracticesAs most NG tubes are placed in at this stage, they are usually deployed solely for the purpose of feeding patients who cannot take in food by mouth. Here is a step-by-step procedure of nasogastric tube feeding:
Preparation of the Feeding Solution: The administration of the feeding formula to the patient is prepared by a health practitioner or caretaker according to what the expected requirements for the feeding by the patient would be. Formulas can be bought pre-packaged or mixed from powder, depending on the patient's needs and the doctor's recommendations.
Feeding Method: Feeding through an NG tube can be done in two basic ways: through bolus feeding or continuous feeding.
Bolus Feeding:This method incorporates the use of a syringe where a specific amount of formula is pushed into an NG tube several times in a day. This Synthetic Diet Goes Well with Plant Based Mealtimes.
Continuous Feeding: Here, a feeding pump is used to feed the formula continuously and slowly for several hours. This can be well tolerated by patients, especially those with sensitive tummies.
Administering the Feed: The NG tube utilises gravity for feeding in most cases, as the formula is poured in, and it normally takes a ride in the nasogastric tube. Or, alternatively, the delivery is done by a pump. Caution has to be observed, failure to do so may result in feeding too fast, hence causing discomfort as well as vomiting.
Post-Feeding Care: The residual milk diet should be flushed after feeding to ensure that the formula remains in the turbine thus leading to coiling. Alternate feeding the patient with the tube and propping the head for about 30 – 60 minutes can prevent aspiration.
Complications and Troubleshooting
NG and Ryles tubes are quite safe and efficient methods. However in some cases there may be complications as well and, therefore, these tubes are:
Tube Dislodgement:In case when the Probe is dislodged and the probe must be reinserted by a health care worker.
Clogging:Administering the formula or medication the Reverse Jab Newton’s rule tube will get blocked if not ensured Proper principles follows. Frequent flushing of the small bore tube with water will also reduce this.
Infection:There are some situations which warrant care around the wound site created by the tracheostomy that if this is not done breaches in care may bring about an infection.
Aspiration:Only in some instances does the aspirated formula enter the lungs aspiration pneumonia complication. Proper tube placement and keeping the head of the patient closed sitting position during feeding and after feeding may also minimise this possibility.
ConclusionThe nasogastric as well as Ryles tube is an invaluable adjunct to patients who are not in a position to eat or swallow on their own. These tubes ensure that patients get the care and nutrition they require via feeding, medications, draining the stomach, or enemas, regardless of the purpose of the tubes.
